
win32
I did it for me.
- Mar 26, 2020
- 57
N is a CYP2D6 substrate[1] (it's also a CYP2B6 substrate, but that's unimportant for now). This means a liver enzyme called CYP2D6 deactivates N. If too much of the N gets deactivated too soon, you won't be asleep and sedated and dying anymore. You'll wake up before you've achieved your goal. N also undergoes extensive first-pass metabolism, deactivating some of it before it even reaches your brain. Excessive metabolism of N could result in either a huge waste of money or even more dire consequences, depending on your situation. About 1 in 33 people on this site could have a genetic defect that causes this, or depending on their ethnicity, their chance might be closer to 1 in 9.
This post is not medical advice, nor an encouragement or endorsement of anything, including the use of N, specific opioids, or specific antidepressants. The content is purely informational in nature.
Genetics
Differences in genetics mean some people naturally have very high or very low levels of this enzyme. The vast majority of people either have normal levels, or lower-than-normal levels (lower is better, because the drug is stronger and lasts longer). But a non-trivial number of people have levels of this enzyme so high that we get very little effect from drugs metabolized by CYP2D6, because they get deactivated 2-10+ times faster than normal. These people are called rapid or ultrarapid metabolizers. People with normal or low CYP2D6 enzymes are called extensive or poor metabolizers. The possible range of metabolism speed is very large.
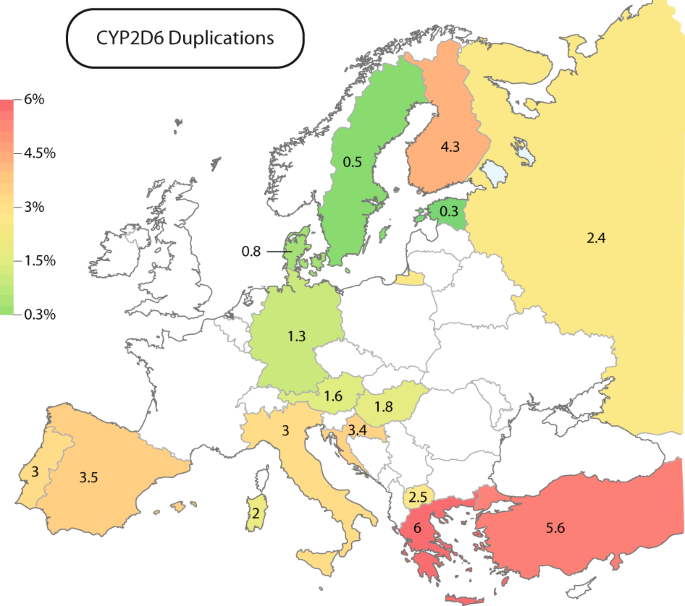
Ultrarapid metabolizer status is associated with certain ethnicities, but anyone of any ethnicity can be an ultrarapid metabolizer. I'm white and an ultrarapid metabolizer, so N is off the table for me. North African, Middle Eastern, and Jewish populations are likelier to be ultrarapid metabolizers. Ethiopians in particular[2] are at risk. Here's a map of Europe[3] showing the % likelihood of CYP2D6 duplication for some countries (rapid/ultrarapid metabolizer status):
How to tell
You can't know for sure without genetic testing. 23andme isn't 100% accurate in all cases unfortunately, but it can detect CYP2D6 polymorphism. You can get your genes tested and and plug the raw data into into an external site like gene2rx for a small additional fee.
You can actually get a general idea based on your response to certain drugs, but this is obviously less reliable. Some drugs are activated by CYP2D6 instead of deactivated by it. These include the opioids codeine, tramadol, and hydrocodone. These drugs are much stronger if you're an ultrarapid metabolizer. If you're like me and you get knocked on your ass and vomit everywhere after taking the smallest Vicodin pill split in half, or tiny amounts of prescription cough syrup fuck you up, it's pretty obvious. Likewise, if these particular opioids do absolutely nothing for you or you require massive doses (without tolerance), it's easy to tell you're a poor metabolizer.
Failure to respond to normal doses of tricyclic antidepressants (no effects and no side effects) and specific SSRIs (paroxetine, fluoxetine) also suggests ultrarapid metabolizer status. Specifically, look for a complete lack of sexual side effects (as these are the most obvious) after a week on the starter dose of paroxetine or fluoxetine as an indicator of ultrarapid metabolizer status.
Potentiation
This is somewhat theoretical, if only because N's 2D6:2B6 affinity is unknown. If it's mostly metabolized by CYP2D6, massive potentiation can be achieved. If CYP2B6 is dominant, there will be only a weak or moderate effect unless you're an ultrarapid metabolizer (although in this case it could also be combined with a CYP2B6 inhibitor). It won't hurt to inhibit CYP2D6 either way, as the chance of success can only be increased by inhibiting this enzyme.
Potentiation of N should be possible with drugs that inhibit the CYP2D6 enzyme. Grapefruit juice won't work here. The Wikipedia page on CYP2D6[4] classifies some CYP2D6 inhibitors, but it's misleading. Some of these are technically correct, but irrelevant due to dosage required, and others only work in vitro (they inhibit the enzyme in dishes, but not in humans).
The most realistic options for strong inhibition are actually antidepressants. Specifically Wellbutrin (bupropion), Paxil (paroxetine), and Prozac (fluoxetine). Getting a prescription for them is trivial. Tagamet (cimetidine) is an OTC non-antidepressant option for moderate inhibition. All of these work best as inhibitors if taken every day for at least a week before N, as their enzyme inhibition effect builds up. Avoid cannabidiol (CBD) and quinine, they're useless here. Also note that the pharmacokinetics involved are complex, and taking one of these is not guaranteed to make N work well for you if you're an ultrarapid metabolizer. It's a more realistic option for normal or poor metabolizers (most people) who want extra security and peace of mind that the N will do its job effectively.
Conclusion
Those without any clues about their CYP2D6 metabolism might want to tread carefully with N, especially if they have North African, Middle Eastern, and/or Jewish blood. It is extremely statistically likely that CYP2D6 ultrarapid metabolism has been responsible for multiple N failures in the past. It has also surely resulted in OD failures involving other drugs such as tricyclic antidepressants; many different drugs are metabolized by CYP2D6. As for CYP2B6, ultrarapid metabolism for this enzyme is incredibly rare (<1%), vs. ~3% overall or >10% in certain populations for CYP2D6. While rapid CYP2B6 metabolism is more common at ~7%, it is (in my non-professional opinion) unlikely to be clinically relevant in a sufficiently large N overdose compared to CYP2D6. I will continue my research into that, however; I could be wrong. If you're worried, do genetic testing.
SN is not metabolized by CYP2D6[5] (or any other CYP enzymes), so it's a safer bet if you belong to a group at high-risk for being an ultrarapid metabolizer.
[1]: https://pubmed.ncbi.nlm.nih.gov/21781739/
[2]: https://pubmed.ncbi.nlm.nih.gov/8764380/
[3]: https://www.nature.com/articles/s41431-019-0480-8
[4]: https://en.wikipedia.org/wiki/CYP2D6
[5]: https://www.mayocliniclabs.com/-/media/it-mmfiles/Special Instructions/B/7/4/Pharmacogenomic_Associations_Tables
This post is not medical advice, nor an encouragement or endorsement of anything, including the use of N, specific opioids, or specific antidepressants. The content is purely informational in nature.
Genetics
Differences in genetics mean some people naturally have very high or very low levels of this enzyme. The vast majority of people either have normal levels, or lower-than-normal levels (lower is better, because the drug is stronger and lasts longer). But a non-trivial number of people have levels of this enzyme so high that we get very little effect from drugs metabolized by CYP2D6, because they get deactivated 2-10+ times faster than normal. These people are called rapid or ultrarapid metabolizers. People with normal or low CYP2D6 enzymes are called extensive or poor metabolizers. The possible range of metabolism speed is very large.
Ultrarapid metabolizer status is associated with certain ethnicities, but anyone of any ethnicity can be an ultrarapid metabolizer. I'm white and an ultrarapid metabolizer, so N is off the table for me. North African, Middle Eastern, and Jewish populations are likelier to be ultrarapid metabolizers. Ethiopians in particular[2] are at risk. Here's a map of Europe[3] showing the % likelihood of CYP2D6 duplication for some countries (rapid/ultrarapid metabolizer status):
How to tell
You can't know for sure without genetic testing. 23andme isn't 100% accurate in all cases unfortunately, but it can detect CYP2D6 polymorphism. You can get your genes tested and and plug the raw data into into an external site like gene2rx for a small additional fee.
You can actually get a general idea based on your response to certain drugs, but this is obviously less reliable. Some drugs are activated by CYP2D6 instead of deactivated by it. These include the opioids codeine, tramadol, and hydrocodone. These drugs are much stronger if you're an ultrarapid metabolizer. If you're like me and you get knocked on your ass and vomit everywhere after taking the smallest Vicodin pill split in half, or tiny amounts of prescription cough syrup fuck you up, it's pretty obvious. Likewise, if these particular opioids do absolutely nothing for you or you require massive doses (without tolerance), it's easy to tell you're a poor metabolizer.
Failure to respond to normal doses of tricyclic antidepressants (no effects and no side effects) and specific SSRIs (paroxetine, fluoxetine) also suggests ultrarapid metabolizer status. Specifically, look for a complete lack of sexual side effects (as these are the most obvious) after a week on the starter dose of paroxetine or fluoxetine as an indicator of ultrarapid metabolizer status.
Potentiation
This is somewhat theoretical, if only because N's 2D6:2B6 affinity is unknown. If it's mostly metabolized by CYP2D6, massive potentiation can be achieved. If CYP2B6 is dominant, there will be only a weak or moderate effect unless you're an ultrarapid metabolizer (although in this case it could also be combined with a CYP2B6 inhibitor). It won't hurt to inhibit CYP2D6 either way, as the chance of success can only be increased by inhibiting this enzyme.
Potentiation of N should be possible with drugs that inhibit the CYP2D6 enzyme. Grapefruit juice won't work here. The Wikipedia page on CYP2D6[4] classifies some CYP2D6 inhibitors, but it's misleading. Some of these are technically correct, but irrelevant due to dosage required, and others only work in vitro (they inhibit the enzyme in dishes, but not in humans).
The most realistic options for strong inhibition are actually antidepressants. Specifically Wellbutrin (bupropion), Paxil (paroxetine), and Prozac (fluoxetine). Getting a prescription for them is trivial. Tagamet (cimetidine) is an OTC non-antidepressant option for moderate inhibition. All of these work best as inhibitors if taken every day for at least a week before N, as their enzyme inhibition effect builds up. Avoid cannabidiol (CBD) and quinine, they're useless here. Also note that the pharmacokinetics involved are complex, and taking one of these is not guaranteed to make N work well for you if you're an ultrarapid metabolizer. It's a more realistic option for normal or poor metabolizers (most people) who want extra security and peace of mind that the N will do its job effectively.
Conclusion
Those without any clues about their CYP2D6 metabolism might want to tread carefully with N, especially if they have North African, Middle Eastern, and/or Jewish blood. It is extremely statistically likely that CYP2D6 ultrarapid metabolism has been responsible for multiple N failures in the past. It has also surely resulted in OD failures involving other drugs such as tricyclic antidepressants; many different drugs are metabolized by CYP2D6. As for CYP2B6, ultrarapid metabolism for this enzyme is incredibly rare (<1%), vs. ~3% overall or >10% in certain populations for CYP2D6. While rapid CYP2B6 metabolism is more common at ~7%, it is (in my non-professional opinion) unlikely to be clinically relevant in a sufficiently large N overdose compared to CYP2D6. I will continue my research into that, however; I could be wrong. If you're worried, do genetic testing.
SN is not metabolized by CYP2D6[5] (or any other CYP enzymes), so it's a safer bet if you belong to a group at high-risk for being an ultrarapid metabolizer.
[1]: https://pubmed.ncbi.nlm.nih.gov/21781739/
[2]: https://pubmed.ncbi.nlm.nih.gov/8764380/
[3]: https://www.nature.com/articles/s41431-019-0480-8
[4]: https://en.wikipedia.org/wiki/CYP2D6
[5]: https://www.mayocliniclabs.com/-/media/it-mmfiles/Special Instructions/B/7/4/Pharmacogenomic_Associations_Tables
Last edited:
